Do you have tight hamstrings? Do you stretch them only to find that you’re not any closer to the suppleness that you desire in those posterior hip extenders? Have you tweaked/pulled your hamstring (due to your tightness maybe...)? Do you feel they’re tighter than Gringotts Bank Security?
Today, we’ll go over some of the reasons why the hamstrings might be tight and in part 2 we’ll go over some of the prevention/rehabilitation techniques to deal with hamstring tweaks.
You may be surprised to find that your tight hamstrings are not actually tight… That sounds like something Professor Dumbledore might say.
Below are some of the potential culprits of “tight” hamstrings. (You’ll see why I put “tight” in quotation marks at the end.)
1. Protective tension.
This is when the brain is telling the hamstrings to remain “on,” for one reason or another, and it creates a sensation of tightness when the hamstrings are stretched. Why does this happen? I’m actually a good example of this. I have congenital laxity (meaning my joints are loose and I’m rather flexible) but for a period of about 3 years, my hamstrings were constantly tight and I could feel them being tugged on every time I bent over, and because of my laxity -and a lifetime of NEVER feeling tight- this was as odd as Hagrid’s love for horribly frightening beasts.
Here’s what was happening: my pelvis tilted, wildly I might add, anteriorly (forward).
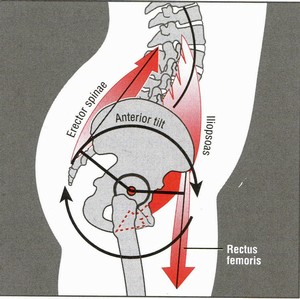
The hamstrings attach to the (posterior) bottom of the pelvis (your “sit” bones) and my brain sensed the constant pelvic tilt and was desperately trying to prevent me tilting forward anymore by firing my hamstrings continually in an attempt to pull my pelvis back into a neutral position. That pelvic tilt results in instability throughout the lower back and pelvis. The brain HATES it when the body is unstable and will do anything necessary to regain stability, which in this case was locking down those hamstrings tighter than a Full Body-Bind Curse.
How do you fix APT? Through lots of dedicated anterior core work (i.e. plank variations) and glute strength. Once my pelvic tilt was in a more neutral position… voilaThe tightness was gone. So, if your hamstrings feel tight, check our your pelvic alignment. Stretching the hamstrings will NOT improve your flexibility in this case; they're already stretched to the max!
2. Neural tension.
I know this will sound similar to the above reason, but this particular tension generally results from an injury. The most likely answer is an injury to a lower back disc. (since the nerve for the hamstrings runs through that region.) If there’s damage to a disc in the L1-S1 region, there’s potentially compression on the nerve for the hamstrings which could result in mishaps in the neural messages (communication between brain and muscles) causing hamstring tightness. Usually this type of tension is accompanied by other symptoms such as tingling, shooting pain, electric pain or numbness. Two common tests to check for spinal issues are the slump test and the heel drop test (which consists of standing on your toes then dropping to you heels. If pain occurs, congratulations! You might have a compression issue.)
3 and 4. Nasty fibrotic tissue or tendonosis in the hamstring.
Sometimes muscle fibers get junky and gunky, from poor movements, overuse, or prior injury, -or all of the above- which changes the length and function of the muscle. Instead of the muscle fibers running parallel and working harmoniously, they’re twisted up like spaghetti noodles (and work as well together and a plate of spaghetti). Soft tissue work such as SMR or possibly work by a professional is in order to help restore the tissue quality.
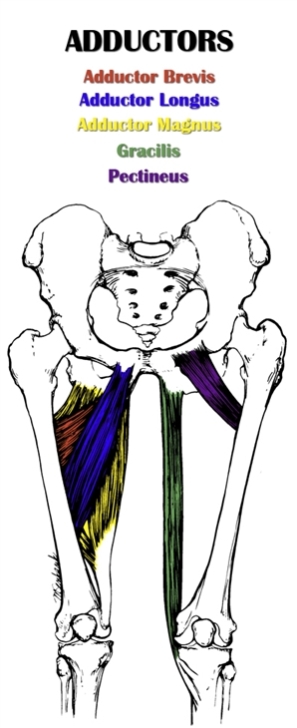
Other areas to target for soft tissue would would be the adductors (since they attach to the pelvis as well) and those fellas are Gunk-City in a lot of folks.
5. The hamstring muscles are truly short.
Yep, they're are people out there either because of their genes (not their jeans. Ha!) or a surgery where the hamstring was immobilized in a shortened position (though this is not common), their hamstrings are physically shorter than they should be. This can happen over time (but to a small-ish degree) in folks who sit down a lot during the day because the pelvis is tilted posteriorly (tucking your butt under) which does shorten the hamstrings a bit. However, this probably isn’t the main source of tightness since they are only short at the very end range of motion.
So what have we learned? If your hamstring is tight, it’s not necessarily it’s fault nor will endless hamstring stretches change anything (even if you’re drew the genetic short stick. Stretching won’t do that much. Sorry.). Soft tissue work in the hamstrings, adductors, and glutes as well as some dedicated anterior core work and glute training (*cough* swings *cough*) can help to solve some tight hamstring issues.
Check back in next week for some hamstring injury causes and care.